The three Clinical Commissioning Groups have been working in partnership with social care commissioners, acute and community services providers, GPs and the stroke Association to look at the best options for patients in stroke hyper-acute, acute and rehabilitation services.
Current stroke services in Coventry and Warwickshire are providing a good standard of care but they are not meeting national guidance and offer different levels of care depending on where you live in the area. We need to address this inequity in the current service and a number of other concerns below:
Inequity
If someone has a stroke, the first 72 hours are crucial. The quality of care people receive makes all the difference in how well they recover from the stroke, or whether they do recover. Particularly important are the first four to six hours. If people need to have thrombolysis to dissolve a clot, it is best for this to happen within a few hours, expert management to reduce the risk of complications is also critical as then the patient has a greater chance of a better recovery and less disability.
Improvements in stroke and TIA or ‘mini stroke’ care have been made but further work is required so more patients can survive their stroke, and stroke survivors can achieve their best level of recovery. There is currently inequitable provision and some significant service gaps in stroke specialist rehabilitation.
Variety of patient pathways
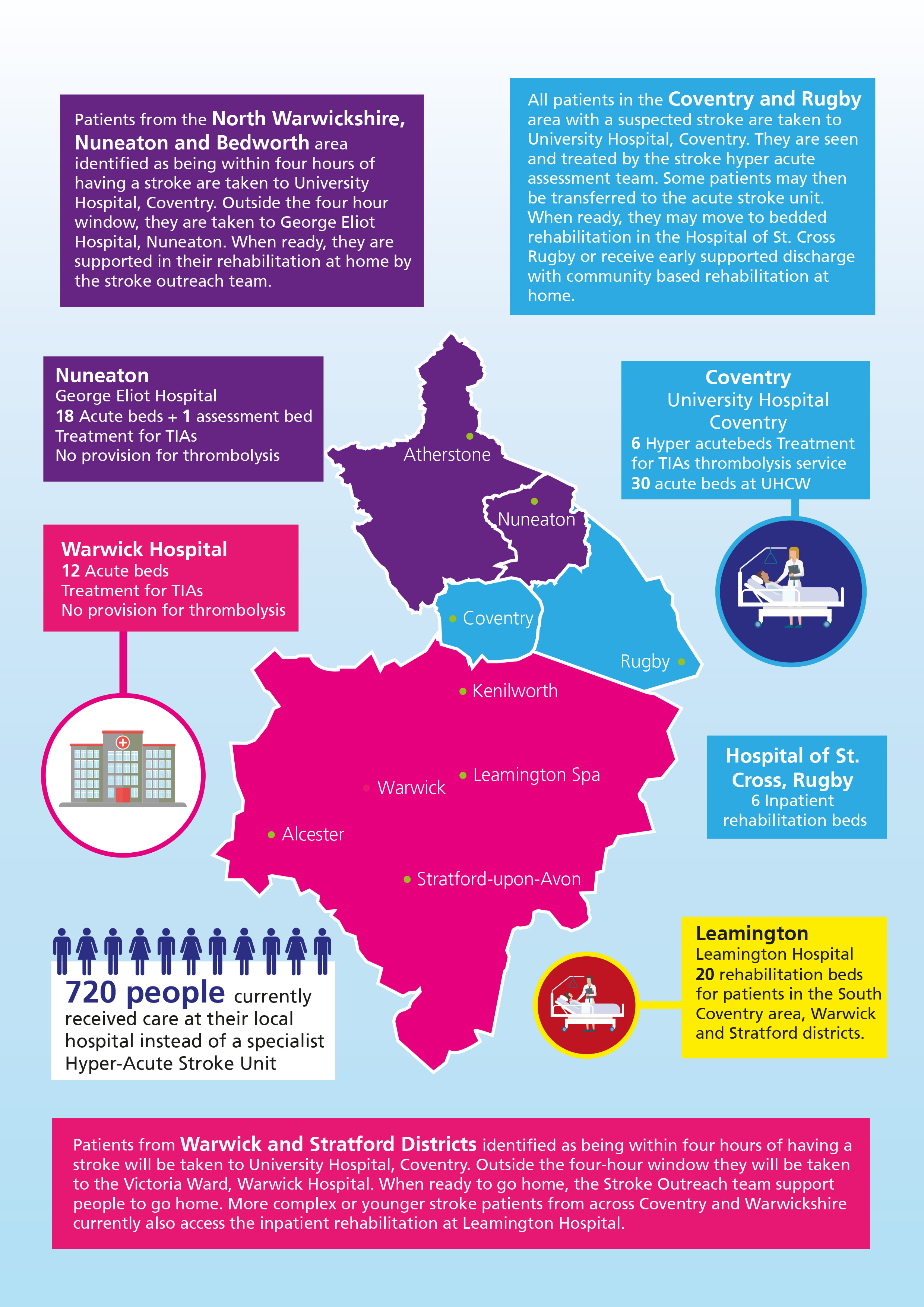
Patients may be moved through the stroke services for diagnosis and treatment in a variety of ways, depending on where they were first taken ill. For example, patients sometimes have to be transferred between hospitals in the early stages of their stroke care for specialist treatment. Some patients can also often stay longer in a main hospital than they need to, when they would be happier and recover more quickly in a community bed or in their own homes, receiving the care they need if that specialist rehabilitation care was available.
Specialist stroke clinicians
We have struggled over many years to recruit stroke specialist doctors and we are aware there is growing evidence of not enough specialist stroke nurses. Our stroke doctors, nurses and therapists are not organised in a way to deliver an integrated, seamless service, because we have not had the best model of service and there are gaps in services. Introducing a better integrated and networked stroke service will help us to recruit, develop and retain the right number of stroke specialists.
Rehabilitation
There are currently three different models for rehabilitation services depending on where you live in Coventry and Warwickshire.
Prevention
Evidence suggests that although we are identifying most, we are not identifying everyone who has atrial fibrillation and who can reduce their risk of stroke by optimising their drug therapy. Early intervention could save around 100 local people a year from having strokes.
The current configuration of services is not giving everyone the best opportunity to survive and where they do, the best opportunity for recovery from a stroke.